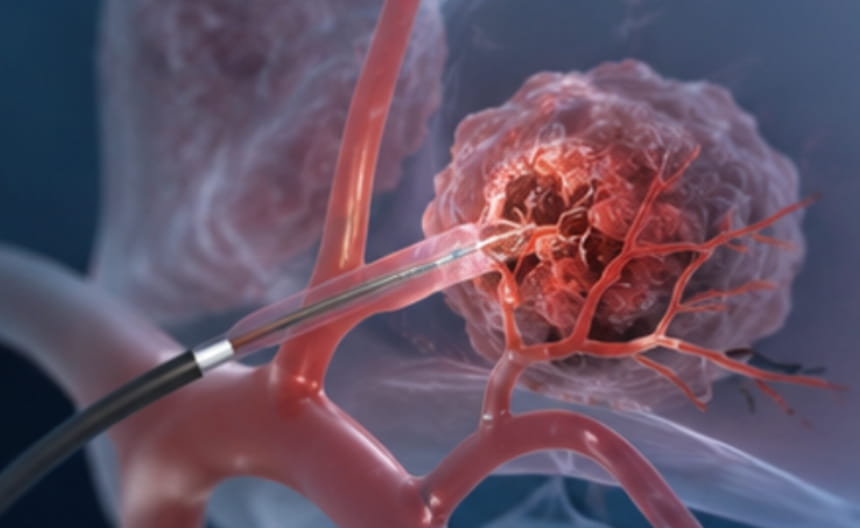
Transarterial intervention is a minimally invasive treatment approach that uses endovascular catheters to deliver therapeutic drugs or embolic agents directly into the arteries supplying a tumor. Depending on the treatment goal and therapeutic strategy, it is mainly classified into three modalities: transarterial infusion chemotherapy, transarterial embolization, and transarterial chemoembolization. These three approaches, each evolving from and complementing the others, together form the foundation of regional therapy for hepatocellular carcinoma and other hypervascular tumors.
Transarterial Infusion chemotherapy (TAI) is an interventional technique in which a microcatheter is superselectively advanced into the main artery supplying the tumor, allowing chemotherapeutic agents to be delivered directly through continuous or pulsed intra-arterial infusion. The principle of TAI is to achieve a dramatically higher local drug concentration within the tumor—often dozens of times greater than that achieved with systemic intravenous chemotherapy—while reducing drug exposure in the systemic circulation and thereby minimizing systemic side effects. TAI is commonly used for palliative tumor reduction and as part of combination therapy for unresectable tumors.
The procedure is performed under real-time angiographic guidance. After the tumor-feeding vessels are clearly identified, the catheter is precisely advanced into the target artery, and chemotherapeutic agents are slowly infused according to the treatment plan. The procedure is minimally invasive and typically requires only a small puncture site, which is compressed after treatment.
High local drug concentration with enhanced efficacy and reduced toxicity: Extremely high drug concentrations can be achieved within the tumor tissue, resulting in stronger anti-tumor effects while significantly reducing systemic side effects.
Superselective and highly targeted: Using superselective microcatheter techniques, therapeutic agents can be delivered directly and precisely to the tumor area, maximizing local drug concentration within the lesion.
Flexible combination and broad applicability: This technique can be used alone or in combination with embolization, ablation, targeted therapy, and immunotherapy to further enhance overall treatment efficacy.
It is primarily used for the palliative treatment of intermediate to advanced-stage primary liver cancer, liver metastases, and hypervascular tumors in areas such as the head, neck, and lungs. It can also be used as postoperative adjuvant chemotherapy to help reduce the risk of local recurrence.
Transarterial Embolization (TAE) is an interventional technique in which embolic agents are selectively delivered through a catheter into the arteries supplying the tumor, mechanically blocking blood flow and thereby inducing tumor ischemia, hypoxia, and ultimately necrosis. Because no chemotherapeutic agents are used during the procedure, TAE is particularly suitable for patients who are unable to tolerate chemotherapy or for clinical situations in which ischemic tumor destruction alone is considered sufficient.
During the procedure, once the tumor-feeding artery is precisely identified, embolic agents such as gelatin sponge particles, polyvinyl alcohol (PVA) particles, or drug-eluting microspheres are injected to block the tumor’s microvascular network directly. After the blood supply is cut off, the tumor tissue gradually undergoes ischemic necrosis, and the tumor mass typically shrinks over time.
Pure ischemic tumor destruction without chemotherapy-related toxicity: This approach avoids the hepatic and systemic side effects associated with chemotherapeutic agents, making it particularly suitable for patients with impaired liver function or those who are unable to tolerate chemotherapy.
Simple and repeatable procedure: As a minimally invasive treatment, embolization can be performed repeatedly or in staged sessions when necessary, allowing flexible adjustment of the treatment schedule.
Broad indications with strong synergistic potential: This technique can be combined with local therapies such as radiofrequency ablation and microwave ablation to help eliminate residual tumor tissue at the treatment margins.
This technique is commonly used for unresectable hepatocellular carcinoma, hepatic hemangioma, hypervascular liver metastases, and emergency bleeding control in selected ruptured liver tumors. It is especially suitable for patients who cannot tolerate chemotherapy or need to preserve remaining liver function.
Transarterial Chemoembolization (TACE) is a combined interventional technique in which a mixture of chemotherapeutic agents and lipiodol is injected into the artery supplying the tumor, followed by embolization to block the vessel. TACE combines the high local drug concentration achieved with Transarterial Infusion Chemotherapy (TAI) and the ischemic tumor-killing effect of Transarterial Embolization (TAE). This approach allows chemotherapeutic agents to remain within the tumor for a longer period, providing sustained anti-tumor activity while simultaneously cutting off the tumor’s blood supply. Through this dual mechanism, TACE produces a synergistic anti-tumor effect and is currently regarded as the standard treatment for intermediate-stage hepatocellular carcinoma according to the Barcelona Clinic Liver Cancer staging system (BCLC) classification.
During the procedure, a chemotherapy–lipiodol emulsion is first slowly infused, allowing the drug-oil mixture to penetrate and fill the tumor microvasculature. Embolic agents, such as gelatin sponge particles, are then administered to further reinforce vessel occlusion. Lipiodol functions not only as an embolic medium but also as a carrier for chemotherapeutic agents and an imaging tracer, helping facilitate postoperative radiological follow-up and treatment assessment.
Dual attack with chemotherapy and embolization: Prolonged local chemotherapy combined with ischemic tumor destruction can result in extensive tumor necrosis after a single treatment session.
Sustained drug release with lower systemic exposure: The lipiodol emulsion enables the slow release of chemotherapeutic agents, prolonging their anti-tumor effect while reducing systemic toxicity.
Well supported by clinical evidence and guideline recommendations: Extensive clinical studies have demonstrated its survival benefits, and it is recognized as a standard first-line treatment for intermediate-stage liver cancer.
It is primarily used for patients with intermediate- to advanced-stage primary liver cancer that cannot be surgically removed. It may also be used as palliative treatment for liver metastases and certain hypovascular tumors. TACE is often combined with ablation, targeted therapy, and immunotherapy to further prolong survival and improve quality of life.