Endometrial cancer is a common malignant tumor of the female reproductive tract, mostly occurring around menopause or after menopause. Because abnormal bleeding often appears early, most patients are diagnosed at a curable early stage, and the overall prognosis is good.
· Obesity, hypertension, and diabetes (the triad)
· Nulliparity
· Polycystic ovary syndrome
· Long-term estrogen therapy
· Genetic factors such as Lynch syndrome
· Tamoxifen use
Long-term unopposed estrogen stimulation is the core driver. Adipose tissue converts androgens into estrogen, aggravating endometrial hyperplasia. People with Lynch syndrome may have a lifetime risk as high as 60%.
The most common symptom is postmenopausal vaginal bleeding or irregular perimenopausal bleeding. Increased vaginal discharge may also occur. Advanced disease may present with pelvic pain, ascites, and other manifestations. Bleeding is an important early signal for seeking medical care.
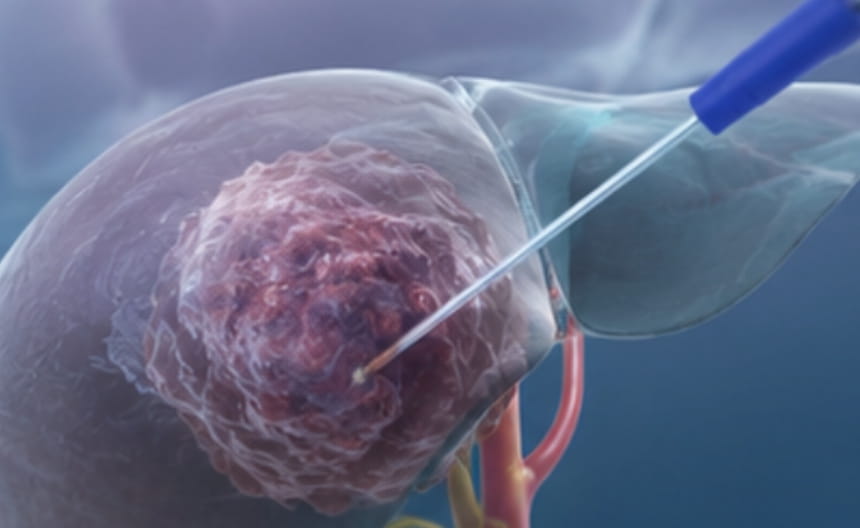
· Surgery: Extrafascial total hysterectomy + bilateral adnexectomy is the first choice, with lymph node dissection determined by pathology. Ovarian preservation may be considered in some young early-stage patients.
· Minimally invasive treatment: Laparoscopic or robot-assisted surgery causes less trauma and allows faster recovery; for fertility preservation, hysteroscopic lesion resection combined with high-dose progestin therapy may be performed.
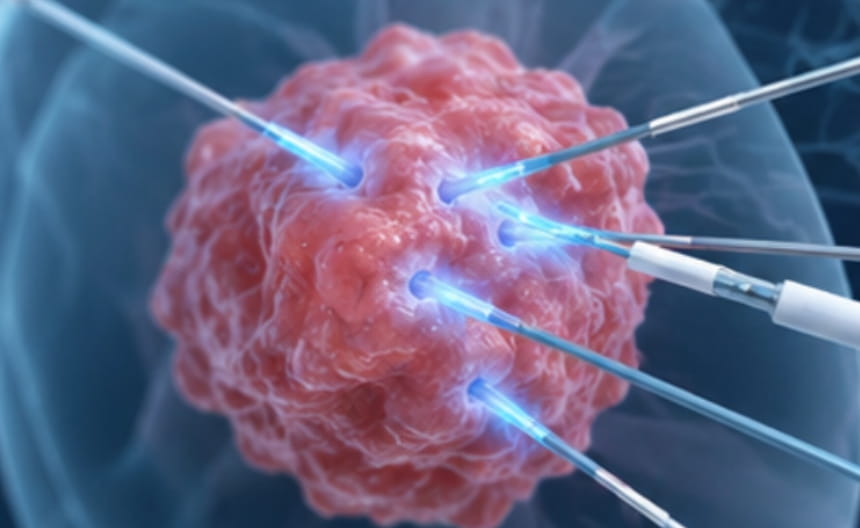
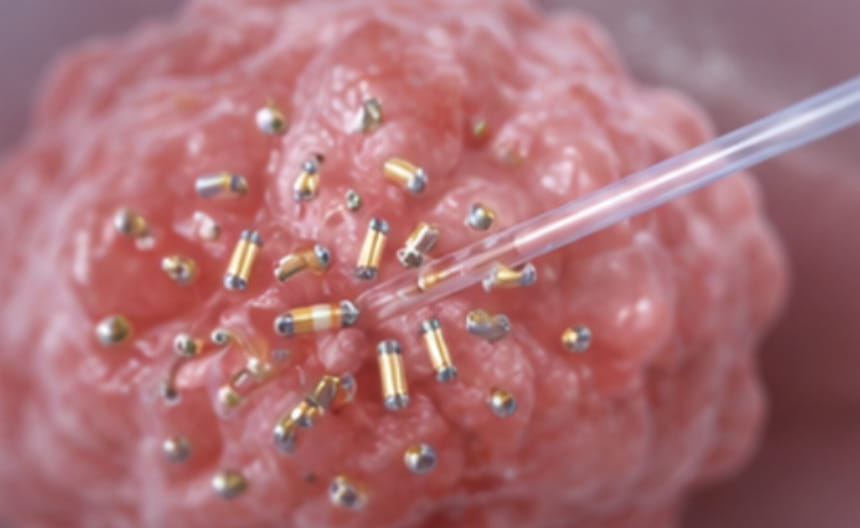
· Chemoradiotherapy: Postoperative adjuvant radiotherapy and chemotherapy are used for high-risk patients; concurrent chemoradiotherapy is used for locally advanced disease.
· Targeted and immunotherapy: Microsatellite instability-high tumors may be treated with immune checkpoint inhibitors; corresponding targeted drugs exist for mutations such as PIK3CA.
· Others: Endocrine therapy (such as progestins) is used for fertility preservation and recurrent disease; genetic counseling guides Lynch syndrome management.
Hysteroscopy with endometrial biopsy is the gold standard. Transvaginal ultrasound measuring endometrial thickness is used for initial screening. MRI evaluates myometrial invasion. CA-125 and imaging are used for staging. Testing for Lynch syndrome-related proteins is recommended.