Ovarian cancer has the highest mortality among gynecologic cancers, with epithelial ovarian cancer being the main type. Because early symptoms are lacking, more than half of patients are diagnosed at an advanced stage. Standardized surgery + chemotherapy + maintenance therapy strategies significantly improve prognosis.
· Genetic mutations such as BRCA1/2 (risk up to 40--60%)
· Early menarche and late menopause
· Nulliparity or late childbirth
· Obesity
· Endometriosis
· Smoking
Repeated injury to the ovarian surface caused by ovulation leads to accumulation of DNA abnormalities in the background of repair gene mutations such as BRCA. The estrogenic internal environment and pelvic inflammation synergistically promote carcinogenesis. Obesity aggravates chronic inflammation.
Early symptoms may include abdominal bloating, increased abdominal girth, early satiety, and abdominal discomfort. As the disease progresses, abdominal pain, urinary frequency and urgency, indigestion, and fatigue may occur. Massive ascites in advanced disease can cause dyspnea, and adnexal masses may be detected on gynecologic examination.
· Surgery: Cytoreductive surgery aims for no visible residual disease and is the cornerstone of treatment. Some patients undergo cytoreduction after neoadjuvant chemotherapy.
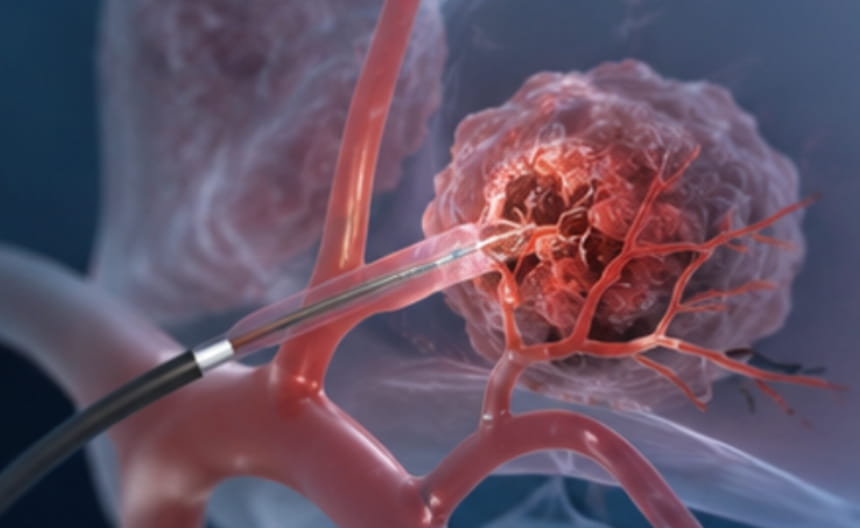
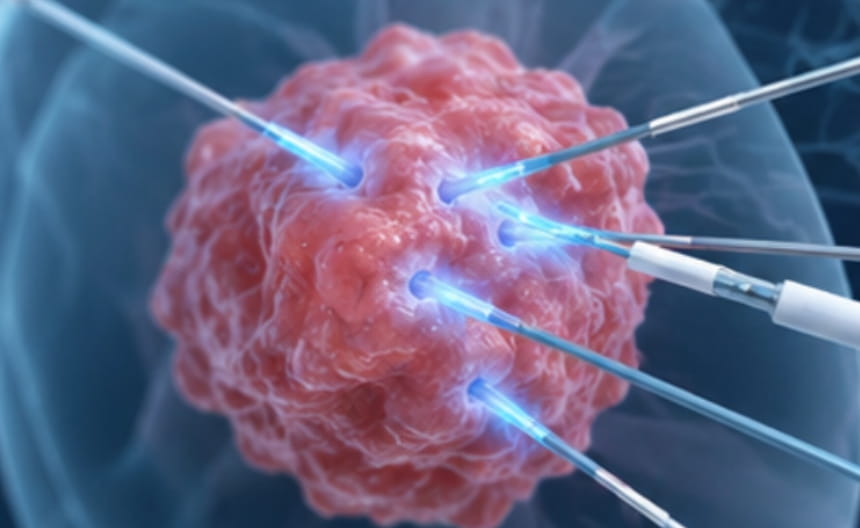
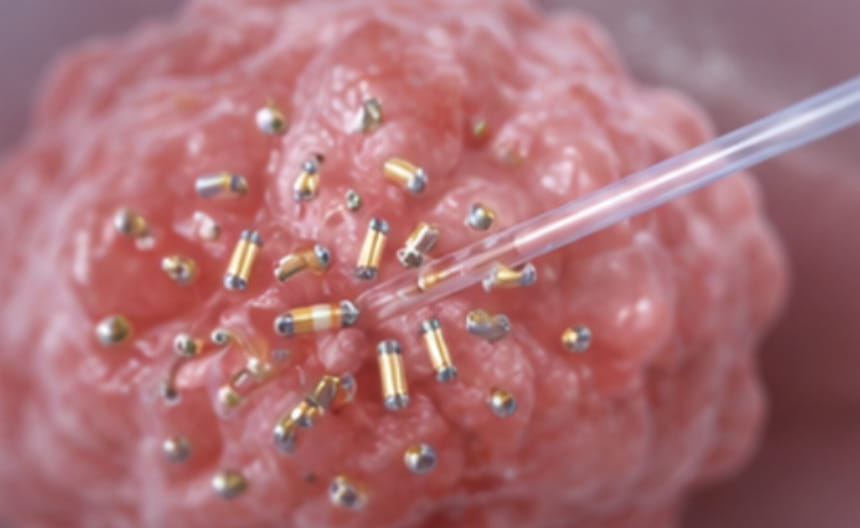
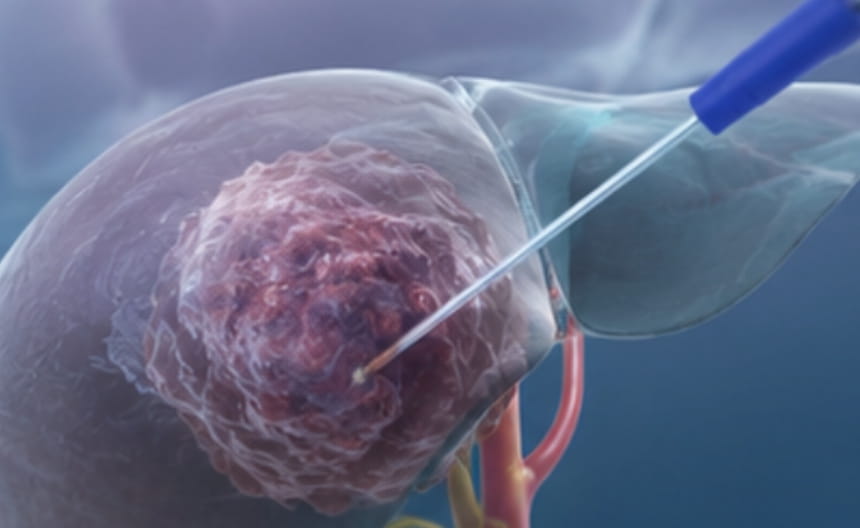
· Minimally invasive treatment: For isolated recurrence or oligometastatic lesions, image-guided radiofrequency ablation or microwave ablation may be considered for local control; radioactive seed implantation may also be used for local treatment.
· Chemoradiotherapy: Postoperative platinum-based chemotherapy is the standard regimen, and hyperthermic intraperitoneal chemotherapy may be used in suitable patients.
· Targeted and immunotherapy: PARP inhibitors are used as maintenance therapy for BRCA-mutated or HRD-positive patients; anti-angiogenic targeted therapy combined with chemotherapy can enhance efficacy.
· Others: Genetic counseling and BRCA testing guide cancer prevention for family members; supportive care improves quality of life.
Pelvic ultrasound is the first choice. Serum CA-125 combined with HE4 assists diagnosis. Contrast-enhanced CT is used for staging. Pathology after surgery defines the subtype. BRCA and HRD testing guide maintenance therapy.