Lymphoma is a heterogeneous group of malignancies originating from the lymphatic and hematopoietic systems, with a complex classification. It is broadly categorized into Hodgkin lymphoma and non-Hodgkin lymphoma. Most subtypes are sensitive to chemotherapy, radiotherapy, and immunotargeted therapies, yielding a relatively high overall cure rate.
· Viral infections such as Epstein-Barr virus (EBV) and human T-lymphotropic virus type 1 (HTLV-1)
· Autoimmune diseases
· Immunodeficiency (HIV, post-organ transplantation)
· Radiation exposure
· Family history of lymphoma and certain chemical exposures
Certain viral infections can induce chromosomal translocations in lymphocytes (such as c-MYC translocation), leading to activation of proto-oncogenes and inactivation of tumor suppressor genes. The immunosuppressive environment promotes uncontrolled lymphoproliferation, and loss of immune surveillance accelerates tumorigenesis.
Painless lymphadenopathy is the most common presentation, most frequently involving the cervical, supraclavicular, axillary, and inguinal regions. Systemic B symptoms include unexplained fever, night sweats, weight loss, and pruritus. Mediastinal lymphadenopathy may cause chest tightness, while intra-abdominal lymphadenopathy can lead to abdominal distension and pain.
· Surgery:Surgery is generally not performed as the primary treatment; excisional lymph node biopsy is undertaken to obtain a complete pathological diagnosis.
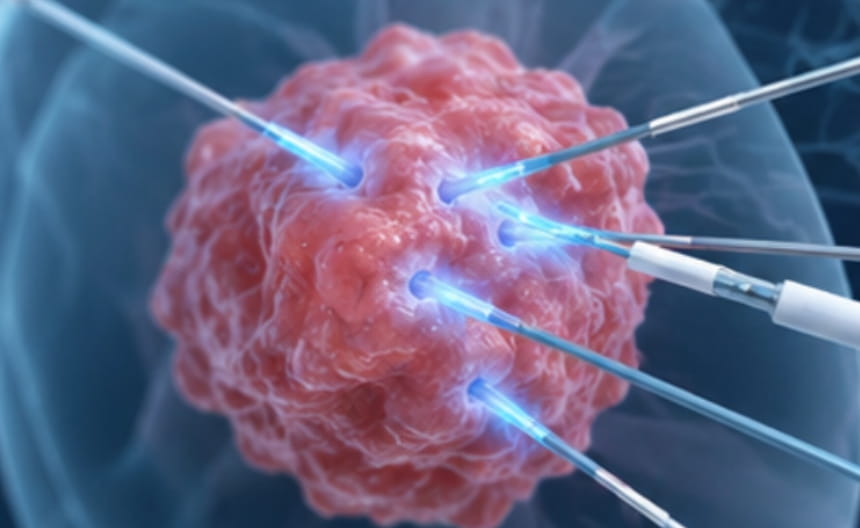
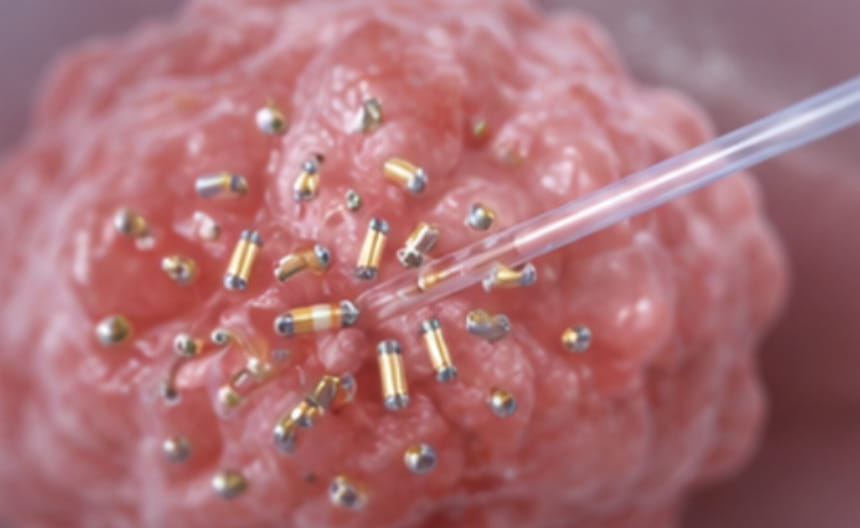
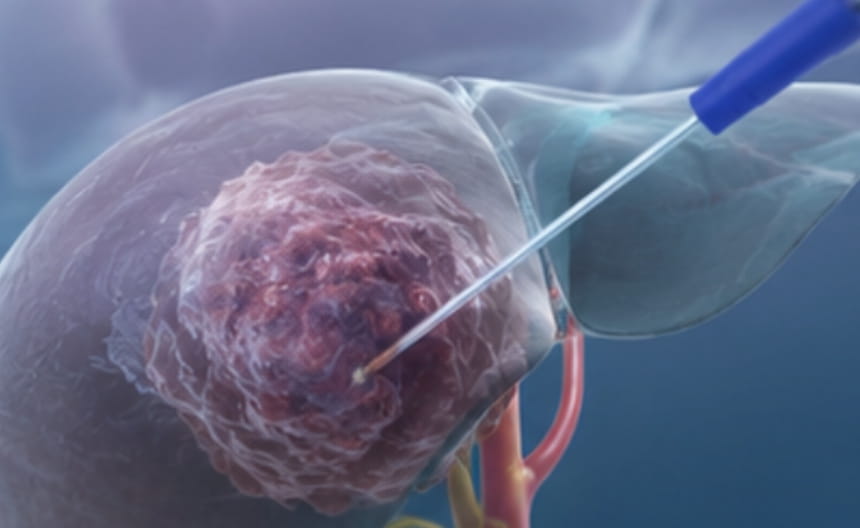
· Minimally invasive therapy:Percutaneous core needle biopsy is used for deep lymph nodes that are difficult to excise. Image-guided radiofrequency ablation or microwave ablation may be employed to manage isolated residual lesions or oligoprogressive extranodal disease.
· Chemoradiotherapy: Chemotherapy serves as the cornerstone of treatment and is combined with conformal radiotherapy for early-stage and localized disease.
· Targeted and immunotherapy: A variety of agents targeting key pathways, antibody-drug conjugates, bispecific antibodies, and CAR-T cell therapies have been applied across various subtypes, achieving high rates of deep remission.
· Other treatments:Autologous or allogeneic hematopoietic stem cell transplantation is used for high-risk and relapsed patients; anti-infective prophylaxis and growth factor support are integrated throughout the treatment course.
Excisional lymph node biopsy is the gold standard for diagnosis; fine-needle aspiration is insufficient for subtyping. PET-CT is an essential tool for staging and response assessment. Bone marrow aspiration and biopsy are performed to evaluate marrow involvement. Flow cytometry and molecular genetic analysis enable precise subtyping.