Renal cell carcinoma arises from the renal tubular epithelium, with clear cell carcinoma being the most common subtype. Early-stage disease is often asymptomatic and is frequently detected during routine physical examination. Localized disease can be cured by surgery, whereas advanced stages require comprehensive treatment with targeted therapy and immunotherapy.
· Smoking (the most widely recognized controllable risk factor)
· Obesity and hypertension
· Hereditary mutations such as von Hippel-Lindau (VHL) syndrome
· Long-term dialysis history
· Diabetes
· Male sex and advancing age
Smoking and obesity lead to oxidative stress and hypoxia-induced gene mutations. Inactivation of the VHL gene is the most common alteration, resulting in accumulation of HIF-α and promotion of angiogenesis. Approximately 3%–5% of cases are hereditary.
The classic triad of hematuria, flank pain, and a palpable abdominal mass is present in only a minority of patients with advanced disease. The more common presentation includes intermittent, painless gross hematuria and dull flank pain. Paraneoplastic syndromes may manifest as fever, hypertension, and hypercalcemia, among others.
· Surgery:For early- and intermediate-stage disease, nephron-sparing partial nephrectomy is performed; radical nephrectomy is indicated when partial resection is not feasible.
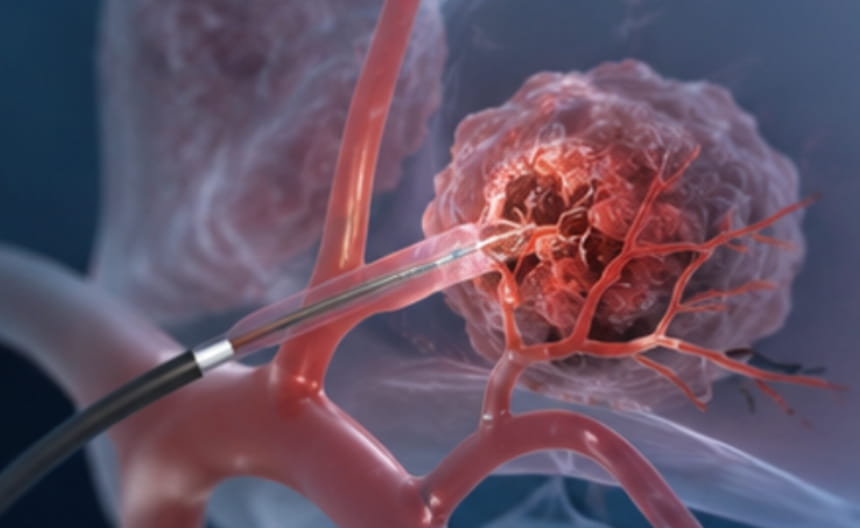
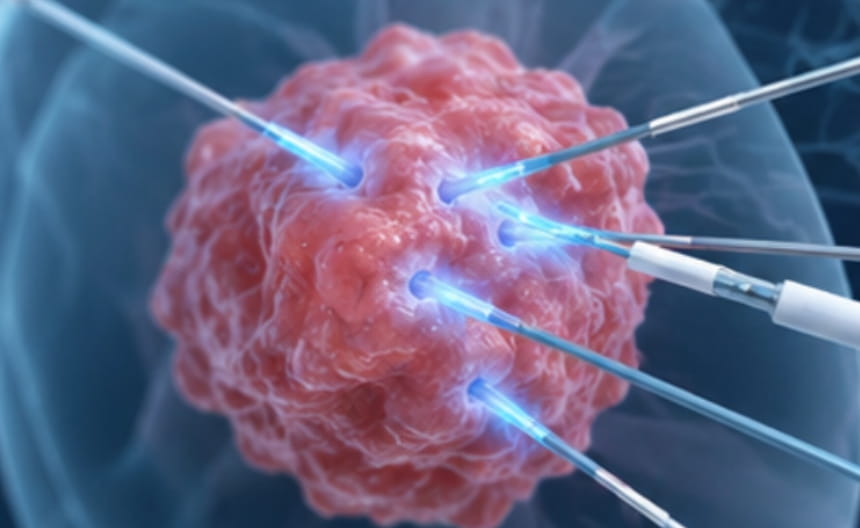
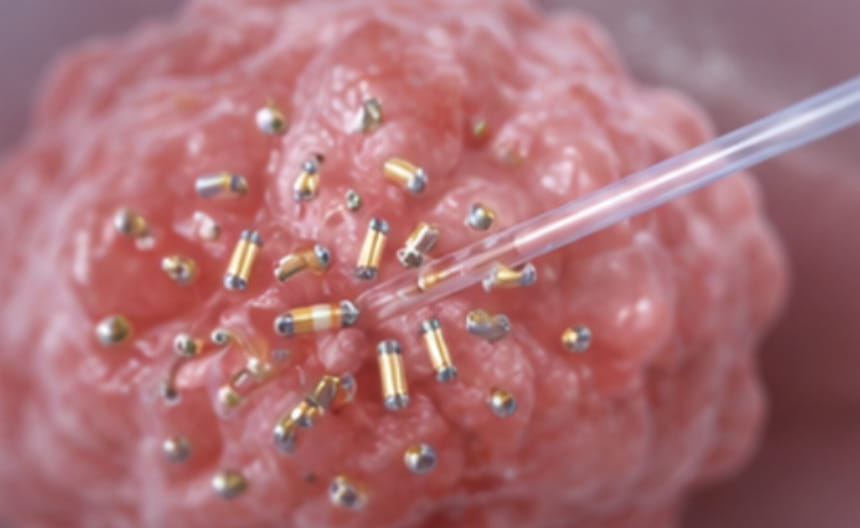
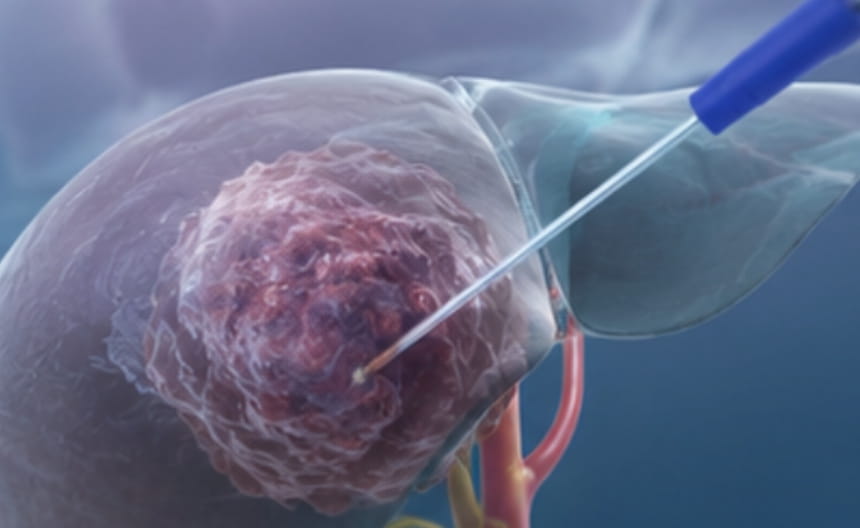
· Minimally invasive therapy:For small renal tumors in patients who are not suitable candidates for surgery, radiofrequency ablation, microwave ablation, or cryoablation may be selected to achieve precise percutaneous tumor destruction. Irreversible electroporation may also be employed to preserve surrounding structures.
· Chemoradiotherapy:Radiotherapy is used for palliative symptom relief in conditions such as bone metastases; conventional chemotherapy has limited efficacy.
· Targeted and immunotherapy: Anti-angiogenic targeted agents combined with immune checkpoint inhibitors represent the standard first-line treatment for advanced disease, significantly prolonging survival.
· Other treatments:Active surveillance is used for low-risk tumors smaller than 2 cm; bone metastases are managed with adjunctive bone-modifying agents.
Contrast-enhanced CT is the gold standard for diagnosis, with early enhancement and rapid washout being the characteristic enhancement pattern. MRI is used for patients with iodine allergies. Percutaneous biopsy is indicated for non-surgical candidates. Chest CT is performed to evaluate pulmonary metastases.