Glioma is the most common primary intracranial malignant tumor and has a very high fatality rate. Prognosis differs greatly between low-grade and high-grade tumors, and molecular classification greatly guides treatment decisions and prognostic assessment.
· High-dose ionizing radiation (the only confirmed environmental factor)
· Genetic syndromes such as neurofibromatosis
· Family history of glioma
· Occupational exposure to certain pesticides and other agents
· Slightly higher incidence in males
IDH1/2 mutations are core drivers of low-grade gliomas and cause genome-wide hypermethylation. Glioblastoma is characterized by EGFR amplification, PTEN deletion, and abundant neovascularization.
Persistent headache (worse in the morning), nausea, vomiting, and other signs of increased intracranial pressure are most common. About 40% of patients develop seizures. Focal neurological deficits such as hemiplegia, speech difficulty, and visual impairment vary by location.
· Surgery: Maximum safe resection is the first choice, with intraoperative navigation, fluorescence guidance, and other aids used to improve resection rates.
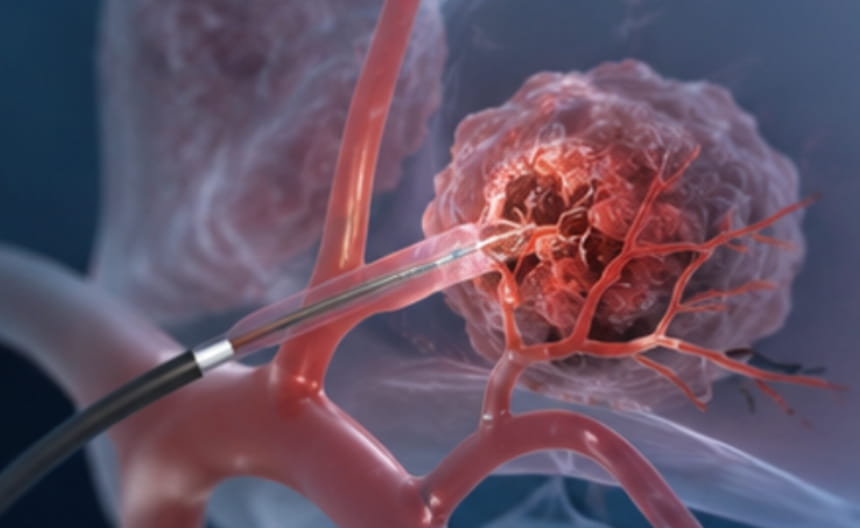
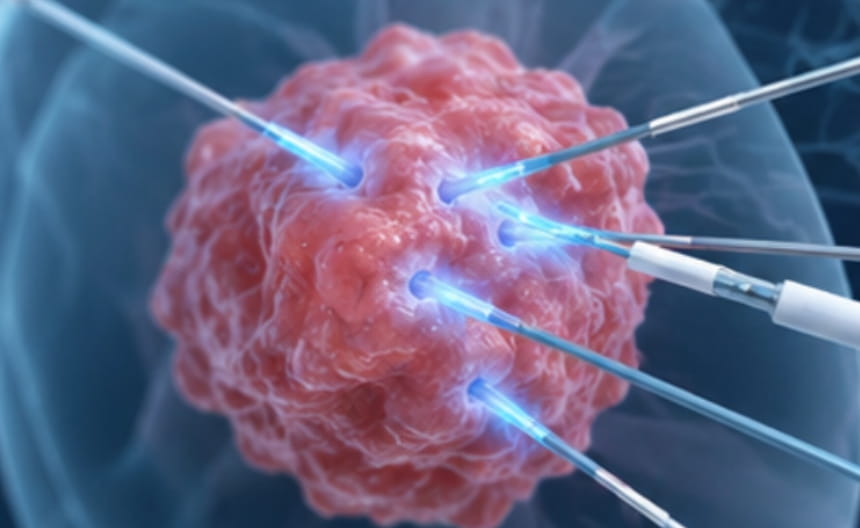
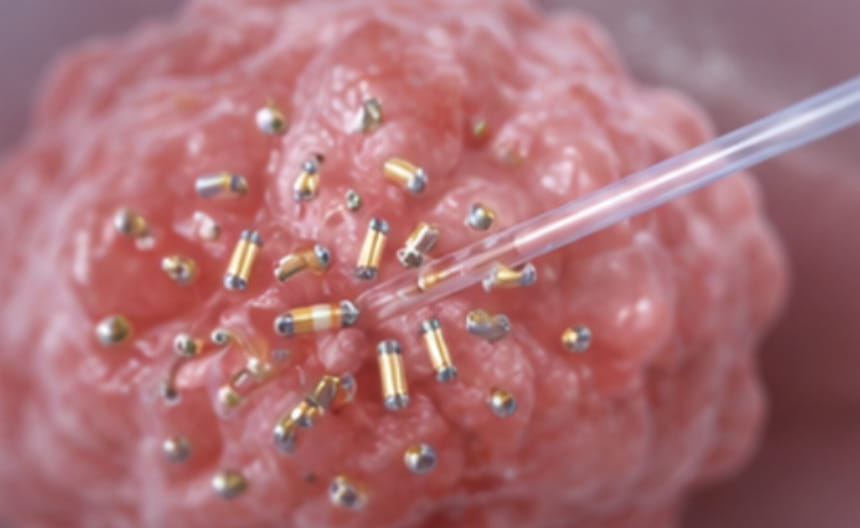
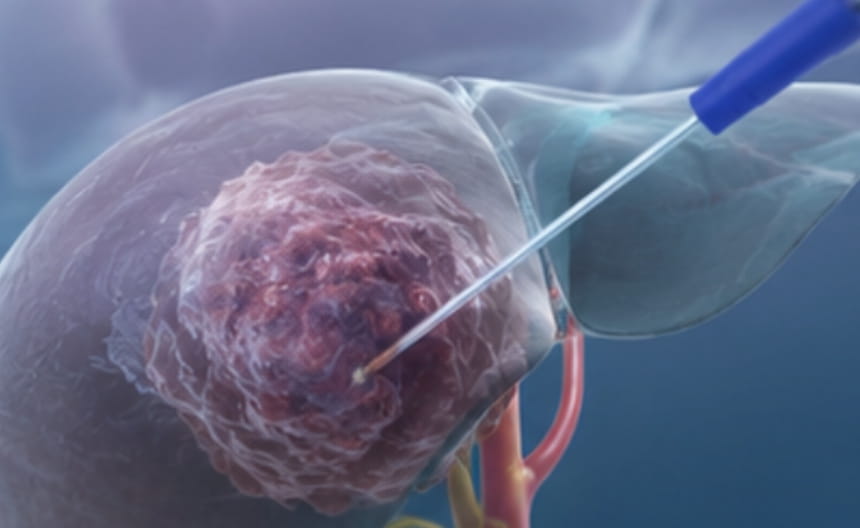
· Minimally invasive treatment: For small deep lesions unsuitable for craniotomy, stereotactic radiosurgery or percutaneous radiofrequency ablation, microwave ablation, and related options may be considered; laser interstitial thermal therapy can serve as a minimally invasive debulking method.
· Chemoradiotherapy: Postoperative concurrent chemoradiotherapy followed by adjuvant chemotherapy is the standard regimen for high-grade gliomas.
· Targeted and immunotherapy: Targeted drugs are selected according to IDH mutation and MGMT methylation status; immune checkpoint inhibitors benefit a small number of cases.
· Others: Tumor treating fields may prolong survival; palliative symptom relief includes steroids to control edema and anti-epileptic therapy.
Contrast-enhanced brain MRI is the first choice, and multimodal imaging assists surgical planning. Stereotactic biopsy obtains pathology, and molecular testing of IDH, 1p/19q, MGMT, and other markers guides treatment.