Gallbladder cancer is the most common highly malignant tumor of the biliary system, with an extremely low 5-year survival rate. Onset is insidious, early symptoms are nonspecific, and most cases are unresectable at diagnosis. Radical surgery is the only potentially curative method.
· Gallstones (present in about 85% of patients)
· Chronic cholecystitis and porcelain gallbladder
· Gallbladder polyps larger than 1 cm
· Anomalous pancreaticobiliary duct junction
· Obesity and high-fat diet
· Genetic susceptibility
Long-term irritation from gallstones causes chronic inflammation and mucosal hyperplasia, while bile stasis leads to accumulation of mutations in genes such as KRAS. Stone size and number are positively correlated with the risk of malignant transformation.
Early symptoms are atypical, including dull right upper abdominal pain and decreased appetite. As the disease progresses, progressive jaundice, pale stools, dark tea-colored urine, pruritus, and a hard palpable mass in the right upper abdomen may occur. Advanced disease is accompanied by ascites and cachexia.
· Surgery: Radical cholecystectomy + liver wedge resection + lymph node dissection is the only potentially curative approach and is suitable for resectable disease.
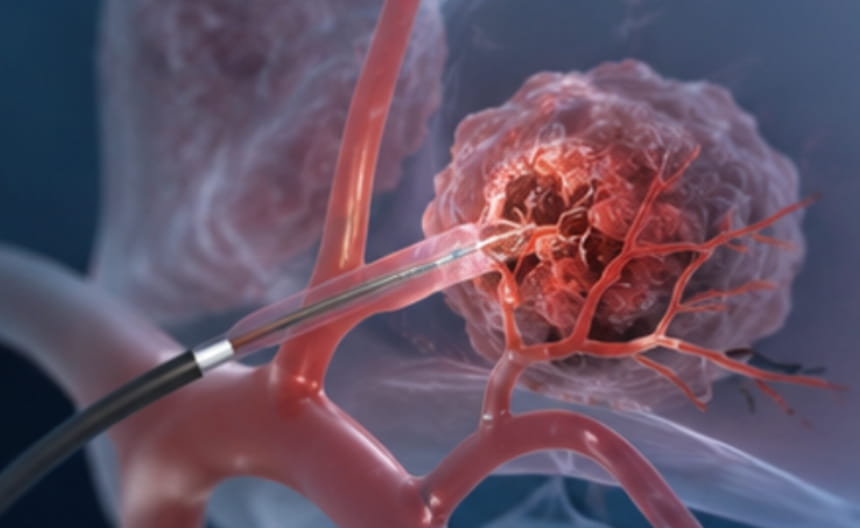
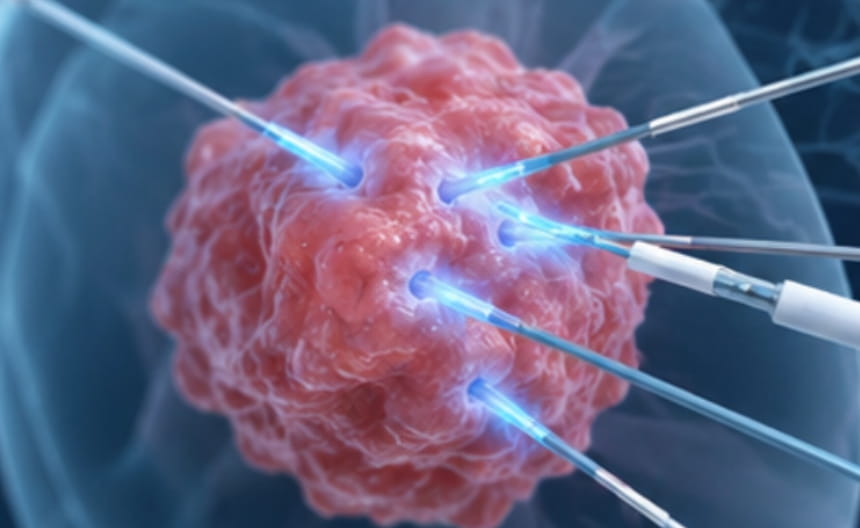
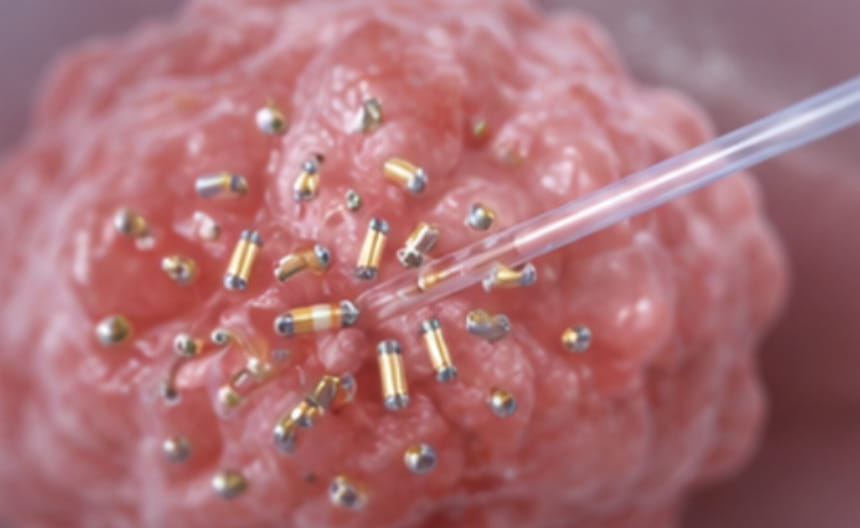
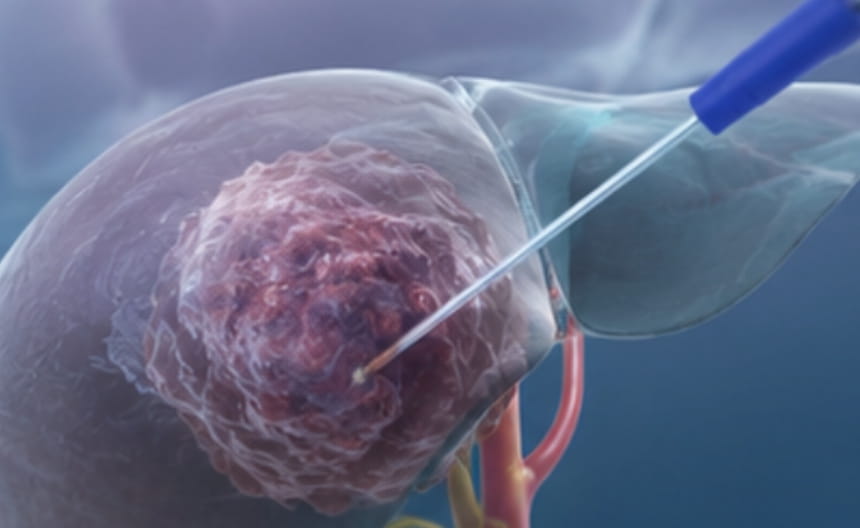
· Minimally invasive treatment: For unresectable disease, endoscopic or percutaneous transhepatic biliary drainage and stent placement can relieve jaundice; intraluminal radiofrequency ablation or photodynamic therapy can control local tumors; limited intrahepatic lesions may be treated with microwave ablation or radioembolization.
· Chemoradiotherapy: Concurrent chemoradiotherapy is used for local control in locally advanced disease; chemotherapy is the foundation for advanced disease.
· Targeted and immunotherapy: Targeted drugs against IDH1 mutations, FGFR2 fusions, and other targets are used in advanced disease; immune checkpoint inhibitors benefit some patients.
· Others: Active jaundice reduction, liver protection, nutritional support, and management of complications such as cholangitis.
Abdominal ultrasound is used for initial screening, and contrast-enhanced CT and MRI assess invasion and metastasis. Magnetic resonance cholangiopancreatography shows biliary morphology. Endoscopic ultrasound-guided needle biopsy confirms the diagnosis. CA19-9 and CEA assist diagnosis.