Cholangiocarcinoma is a rare invasive cancer originating from the bile duct epithelium and is classified by anatomical location as intrahepatic, perihilar, or distal cholangiocarcinoma. Global incidence is increasing, and Asia has relatively high incidence because of factors such as liver fluke infection. The disease has an extremely insidious onset, lacks early signs and effective screening markers, and more than about 65% of patients are unresectable at initial diagnosis, with median survival less than two years. In recent years, however, targeted therapy for specific genetic alterations and minimally invasive jaundice-relieving techniques have brought new opportunities for patients with advanced cholangiocarcinoma.
· Primary sclerosing cholangitis (lifetime cancer risk about 10%~15%)
· Clonorchis sinensis or Opisthorchis viverrini infection
· Congenital choledochal cysts and Caroli disease
· Intrahepatic bile duct stones and recurrent suppurative cholangitis
· HBV or HCV infection and cirrhosis
· Metabolic syndrome, diabetes, and nonalcoholic fatty liver disease
Chronic biliary inflammation causes repeated injury and repair of the bile duct epithelium, leading to accumulation of genetic mutations. The genomic profiles of cholangiocarcinoma differ by location: intrahepatic cholangiocarcinoma commonly shows IDH1/2 mutations and FGFR2 gene fusions, whereas extrahepatic cholangiocarcinoma more often has KRAS and TP53 mutations. Liver flukes cause chronic inflammation through mechanical injury and egg-induced irritation, generating reactive oxygen species and carcinogenic metabolites. In primary sclerosing cholangitis, persistent autoimmune inflammatory signaling pathways remain activated, greatly increasing the probability of malignant transformation.
Extrahepatic cholangiocarcinoma causes progressively worsening painless obstructive jaundice early, with dark tea-colored urine, pale clay-colored stools, and stubborn generalized pruritus. Intrahepatic cholangiocarcinoma often presents with nonspecific symptoms: dull right upper abdominal discomfort, fatigue, decreased appetite, and weight loss; jaundice or a palpable hepatic mass appears only in advanced stages. When complicated by cholangitis, recurrent fever, chills, and right upper abdominal pain occur as a triad.
· Surgery: Radical surgical resection is the only potentially curative method and requires negative margins. Some strictly selected early perihilar cholangiocarcinoma patients may undergo liver transplantation, and combined neoadjuvant chemoradiotherapy can improve efficacy.
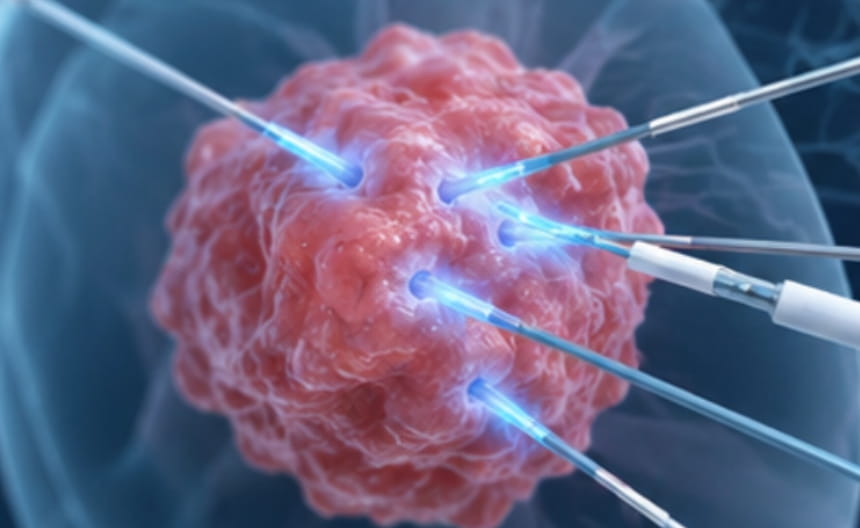
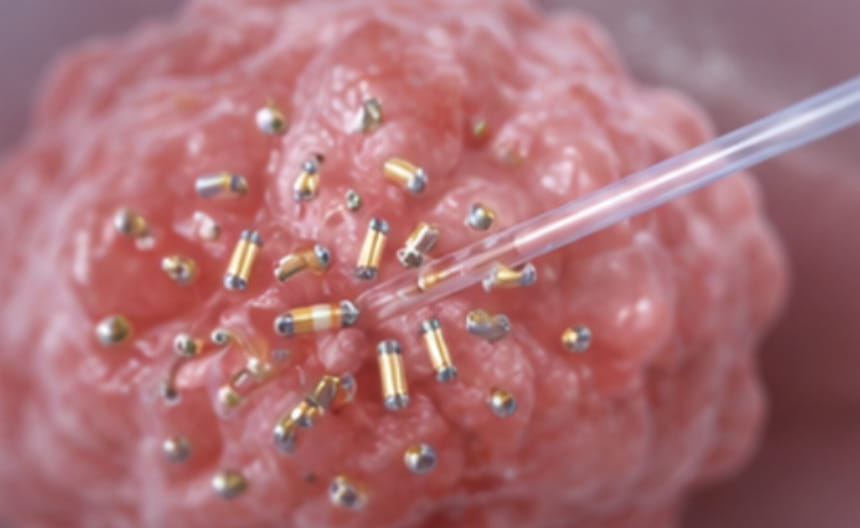
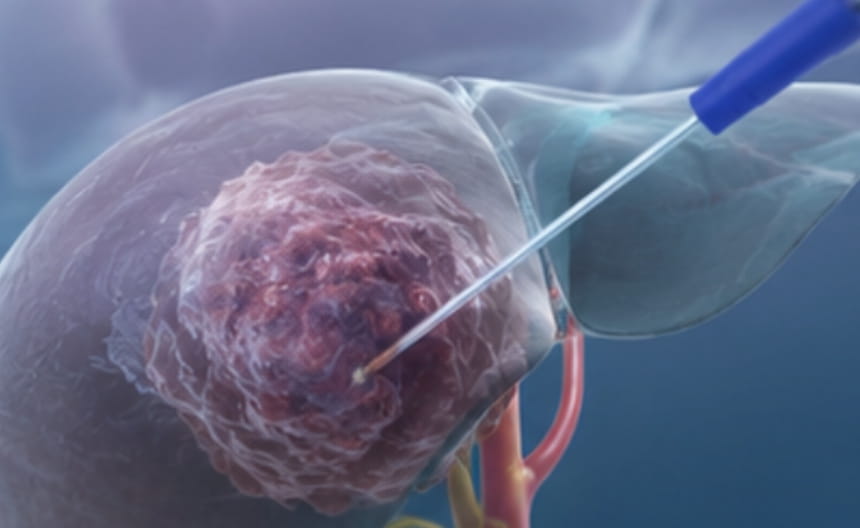
· Minimally invasive treatment: Endoscopic retrograde cholangiopancreatography or percutaneous transhepatic access can place plastic or self-expanding metal stents to immediately relieve biliary obstruction and reduce jaundice. Intraluminal radiofrequency ablation or photodynamic therapy delivers energy through cholangioscopy to locally destroy tumors and prolong stent patency. Limited intrahepatic lesions are suitable for image-guided microwave ablation or hepatic artery radioembolization.
· Chemoradiotherapy: Local concurrent chemoradiotherapy is used for unresectable locally advanced cholangiocarcinoma to control tumor growth and relieve pain. Advanced chemotherapy is based on platinum-containing doublet regimens to prolong survival and improve symptoms.
· Targeted and immunotherapy: Targeted drugs against driver genes such as FGFR2 fusion, IDH1 mutation, and BRAF V600E have been approved for corresponding indications. Immune checkpoint inhibitors show some efficacy in patients with mismatch repair deficiency or high tumor mutational burden.
· Others: Adequate bile drainage, liver protection, infection control, and nutritional support are integrated throughout treatment. Refractory pruritus can be treated symptomatically to improve quality of life.
Magnetic resonance cholangiopancreatography is the preferred noninvasive test and shows bile duct wall thickening, luminal stenosis, or interruption. Endoscopic retrograde cholangiopancreatography and percutaneous transhepatic cholangiography can simultaneously obtain brush cytology or biopsy specimens. Endoscopic ultrasound-guided fine-needle aspiration improves the pathological positivity rate. CA19-9 and CEA are auxiliary diagnostic and follow-up markers, but false positives caused by benign biliary obstruction must be excluded.