Thyroid cancer is the most common malignancy of the endocrine system and occurs more frequently in women. The majority of cases are well-differentiated papillary thyroid carcinoma (PTC), which is associated with an excellent prognosis and is often colloquially referred to as an "indolent cancer" due to its typically slow growth and favorable outcomes. However, anaplastic thyroid carcinoma (ATC) is a highly aggressive subtype with rapid progression and poor prognosis, emphasizing the necessity of timely diagnosis and standardized treatment.
· Exposure to ionizing radiation involving the head and neck during childhood
· Family history of thyroid cancer and presence of RET gene mutations
· Abnormal iodine intake, either excessive or deficient
· Obesity
· Hashimoto's thyroiditis (chronic autoimmune thyroiditis)
Ionizing radiation can induce RET rearrangements or BRAF mutations, leading to activation of the MAPK signaling pathway. Approximately 5%–10% of cases are hereditary, involving a variety of germline genetic mutations. Inappropriate iodine intake promotes thyroid tissue hyperplasia and the accumulation of mutations.
The most common presentation is a painless neck mass that moves with swallowing. When large, it may compress the trachea or esophagus, leading to difficulty breathing or swallowing; invasion of the recurrent laryngeal nerve causes hoarseness. Most cases are detected incidentally during ultrasound examination.
· Surgery:Thyroid lobectomy or total thyroidectomy is the primary curative treatment, with central compartment or lateral neck lymph node dissection performed according to risk stratification.
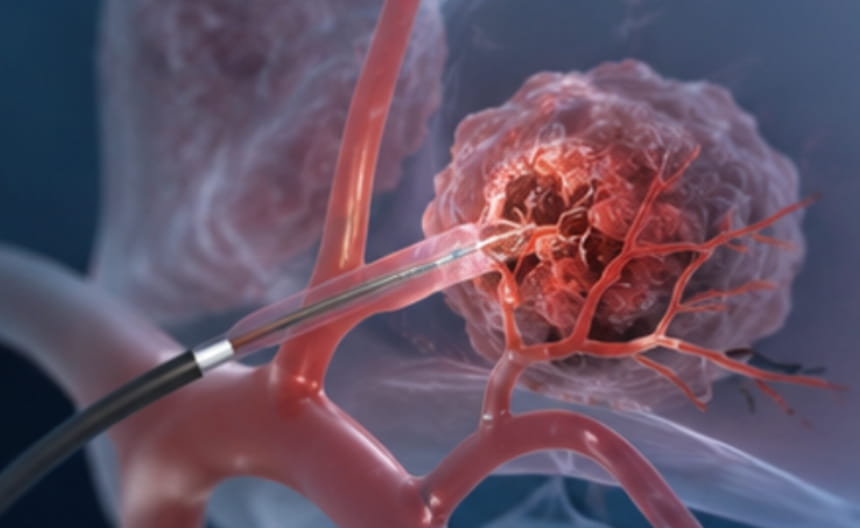
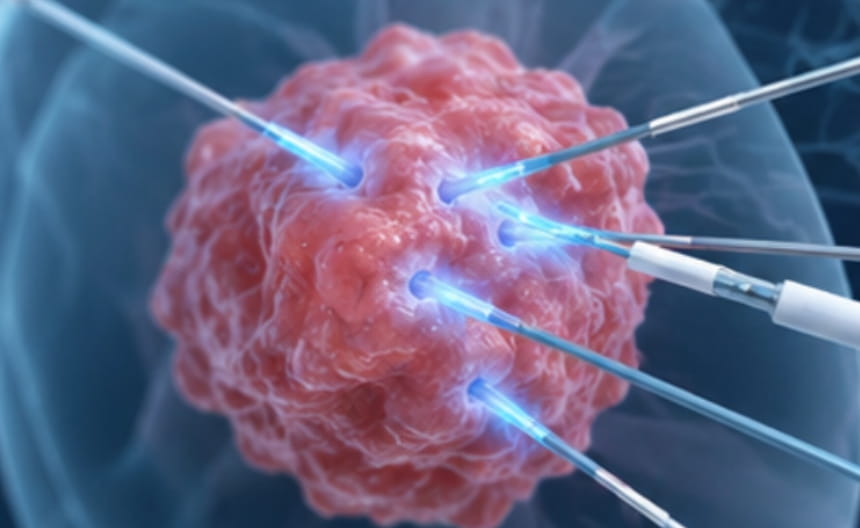
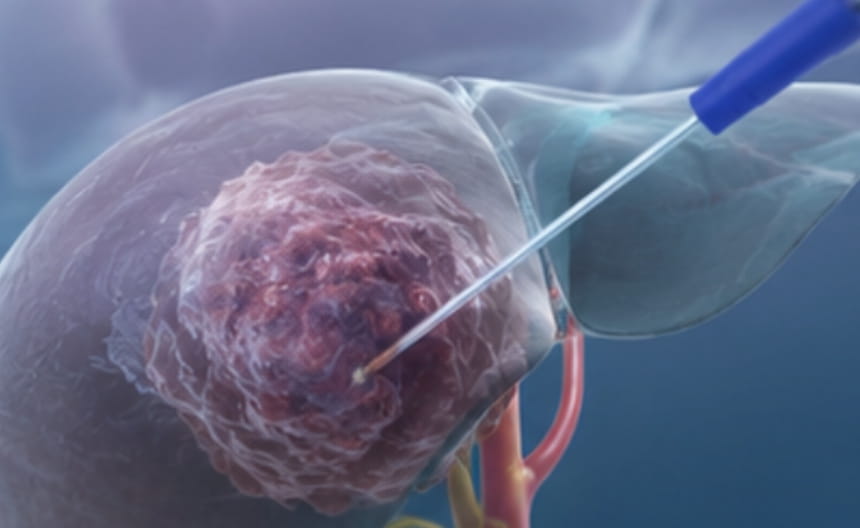
· Minimally invasive therapy:Ultrasound-guided radiofrequency ablation and microwave ablation can be used for microcarcinomas, recurrent lesions, or in patients who are intolerant of surgery; these techniques leave no neck scar and preserve normal thyroid function.
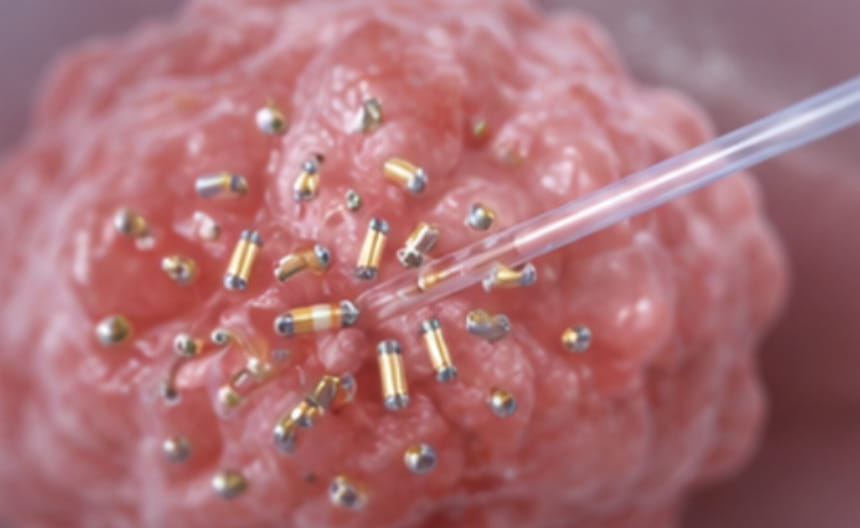
· Chemoradiotherapy: Postoperative radioactive iodine-131 is used to ablate residual thyroid tissue and micrometastases; radiotherapy may be considered for iodine-refractory cases.
· Targeted and immunotherapy:Targeted agents directed against driver genes such as RET and BRAF are used in iodine-refractory advanced cases.
· Other treatments:Thyroid-stimulating hormone (TSH) suppressive therapy maintains low TSH levels to reduce the risk of recurrence.
High-resolution ultrasound combined with TI-RADS grading is used for screening. Ultrasound-guided fine-needle aspiration biopsy confirms the diagnosis. Calcitonin measurement helps exclude medullary thyroid carcinoma. Postoperative monitoring includes thyroglobulin and thyroglobulin antibody levels.