Testicular cancer is the most common solid tumor in young men aged 15--35 years, and most cases are germ cell tumors. It is one of the most curable solid tumors, with 5-year survival exceeding 95% in early-stage patients and also reaching more than 80% in advanced disease.
· Cryptorchidism (the most important risk factor)
· Family history of testicular cancer
· Testicular dysgenesis
· Previous cancer in the contralateral testis
· Ethnic background (higher risk in White populations)
· HIV infection
Abnormal testicular descent during embryonic development disrupts the seminiferous tubule microenvironment and promotes development of carcinoma in situ. Isochromosome of the short arm of chromosome 12 (i12p) is a highly characteristic marker. Genetic polymorphisms are also associated with risk.
The most common presentation is a painless unilateral hard testicular lump or diffuse enlargement with a sense of heaviness. A minority of patients have acute pain due to intratumoral hemorrhage. About 10%--15% first present with symptoms of distant metastasis, such as back pain, cough, or a neck mass. Breast enlargement may result from excessive HCG secretion.
· Surgery: Radical inguinal orchiectomy is the first step in diagnosis and treatment. Retroperitoneal lymph node dissection is performed for stage II non-seminomatous germ cell tumors.
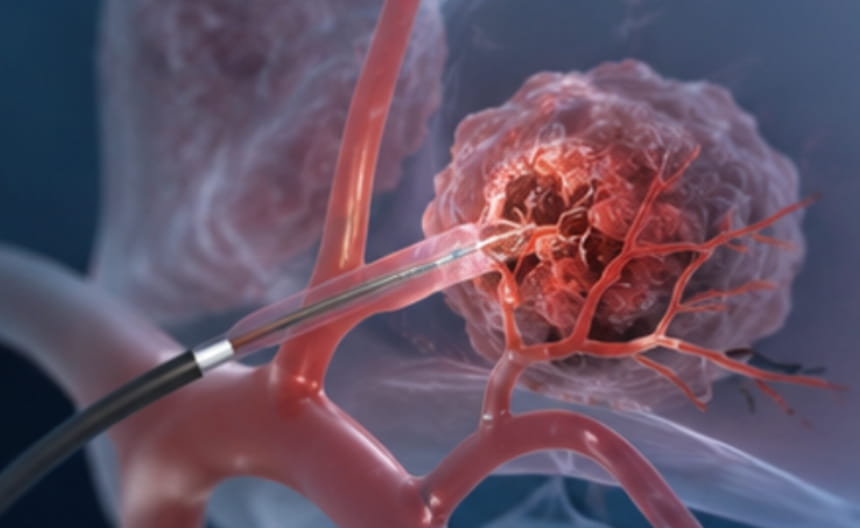
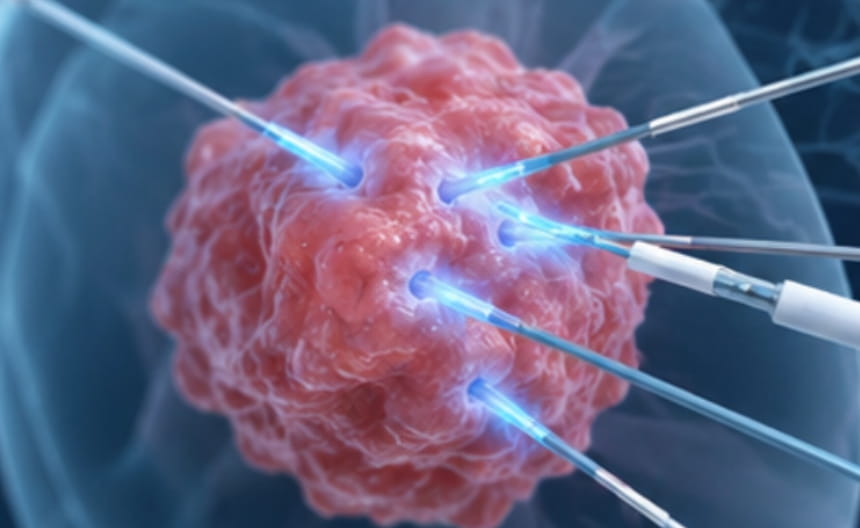
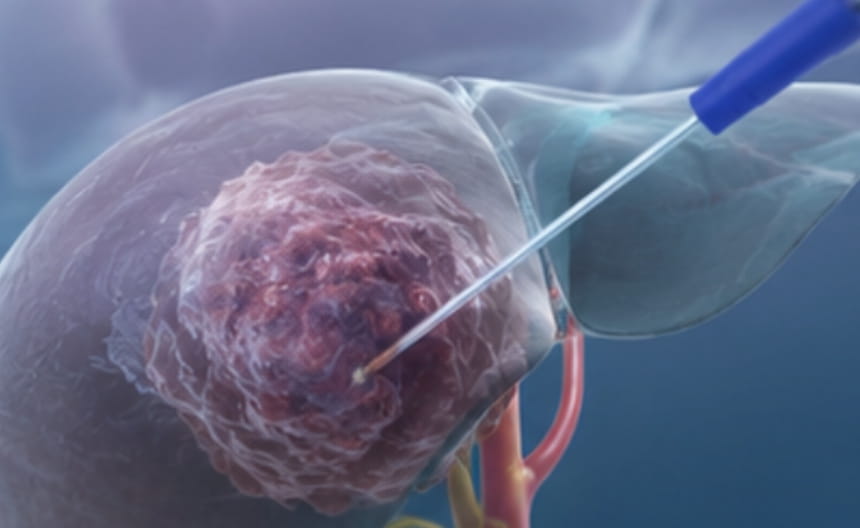
· Minimally invasive treatment: For small residual retroperitoneal lymph nodes or isolated metastases, if repeat surgery is unsuitable, image-guided radiofrequency ablation, microwave ablation, or cryoablation may be considered for local control.
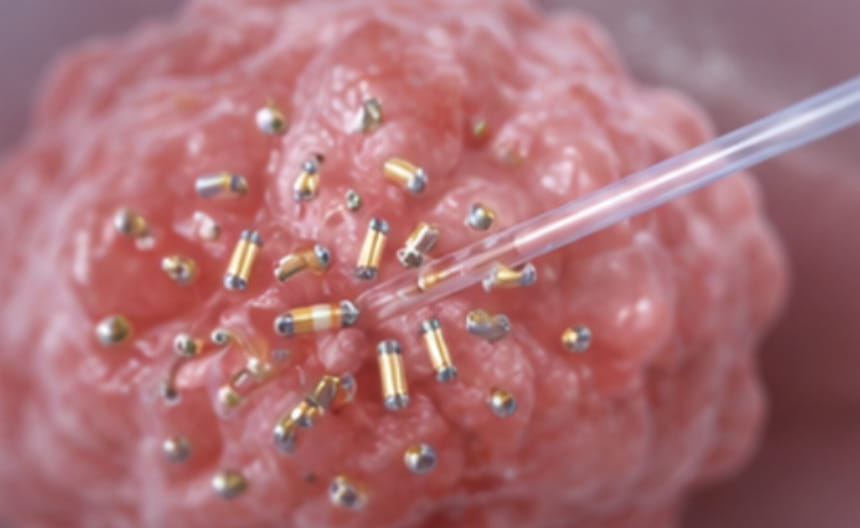
· Chemoradiotherapy: For stage I seminoma, adjuvant radiotherapy or chemotherapy may be selected after surgery; advanced and widely metastatic disease is chemotherapy-based, with a very high cure rate.
· Targeted and immunotherapy: A small number of resistant patients may receive targeted therapy or immune checkpoint inhibitors.
· Others: High-dose chemotherapy combined with stem cell transplantation is used for relapsed and refractory patients; long-term follow-up and endocrine management after treatment are important.
Scrotal ultrasound is the most sensitive screening method. Serum tumor markers AFP, β-hCG, and lactate dehydrogenase should be measured both before and after surgery. Contrast-enhanced CT of the chest, abdomen, and pelvis is used for accurate staging and monitoring.