Pancreatic cancer is an extremely aggressive malignancy, with a 5-year survival rate of less than 10%. Approximately 75%–90% of patients have unresectable disease at the time of diagnosis. Surgery remains the only potentially curative treatment. In recent years, targeted therapy and minimally invasive techniques, particularly nano-knife (irreversible electroporation) surgery, have brought new hope for cure.
·Long-term smoking (the most significant controllable risk factor)
·Obesity and high-fat diet
·Chronic pancreatitis and diabetes
·Hereditary mutations such as BRCA1/2
·Age over 60 and male sex
Smoking induces high-frequency KRAS mutations, and chronic inflammation promotes the accumulation of genetic abnormalities. Hereditary BRCA mutations lead to defective DNA repair, driving malignant transformation of cells, while the fibrotic microenvironment accelerates disease progression.
There are no specific symptoms in the early stage. As the disease progresses, patients may present with persistent epigastric pain radiating to the lower back and progressive painless jaundice (in pancreatic head cancer), accompanied by marked weight loss and loss of appetite. New-onset diabetes may serve as an early diagnostic clue.
· Surgery: Pancreaticoduodenectomy or distal pancreatectomy is performed for resectable cases, followed by adjuvant chemotherapy. For patients with borderline resectable disease, neoadjuvant chemotherapy is administered to increase the likelihood of successful surgery.
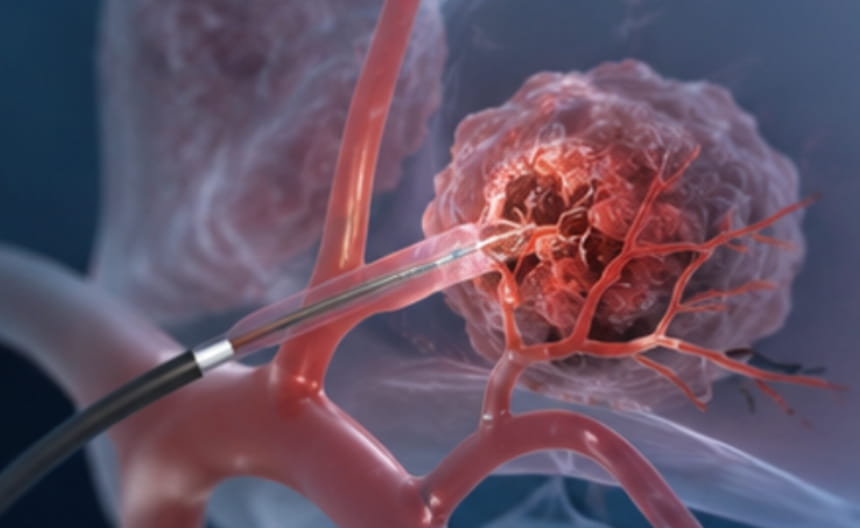
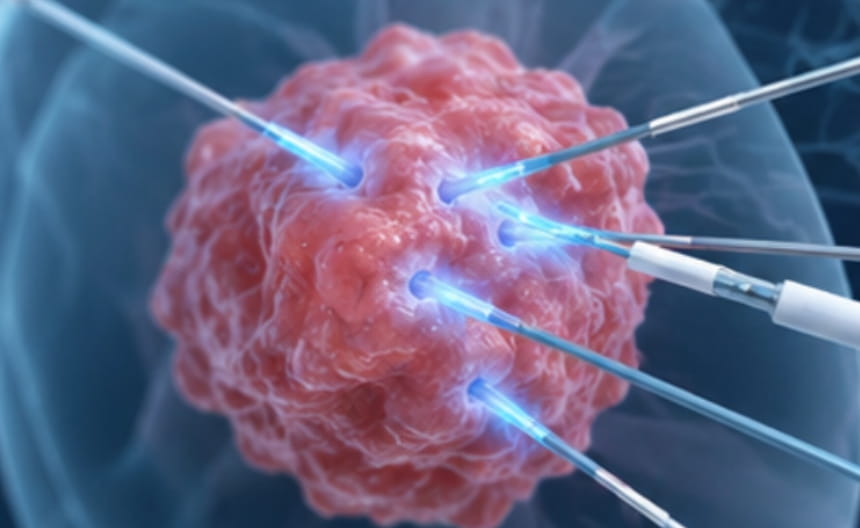
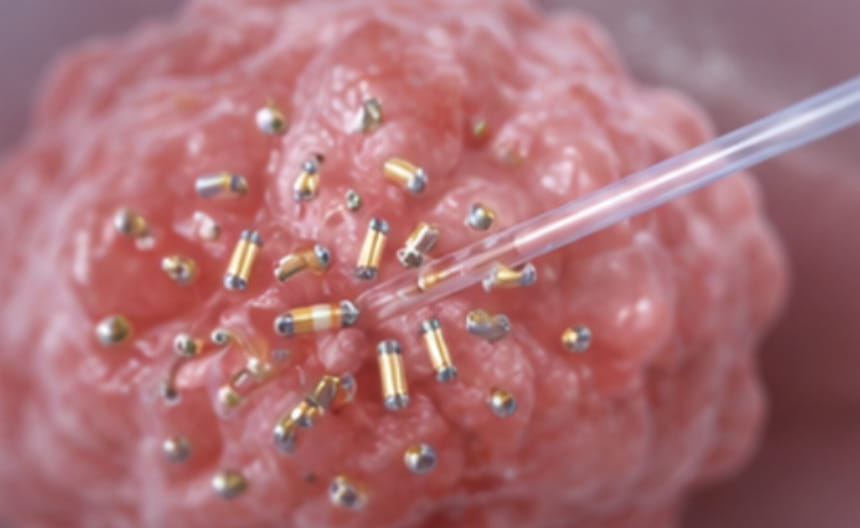
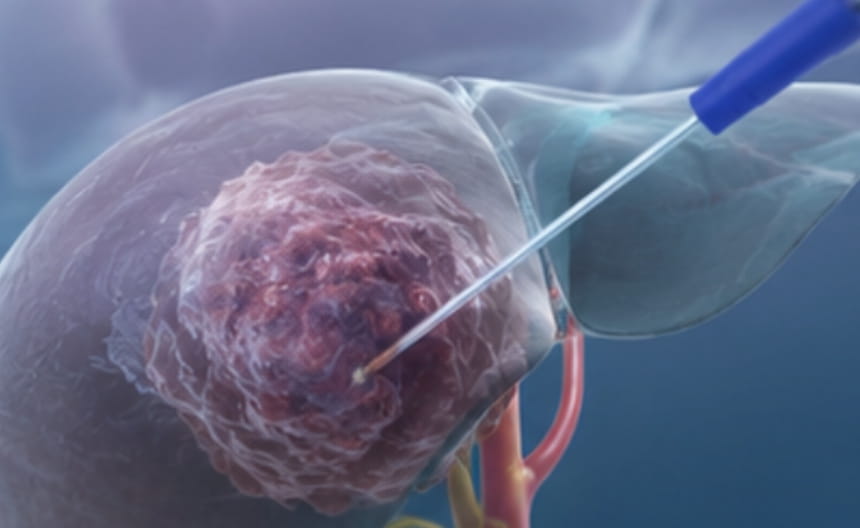
· Minimally invasive therapy:For patients with unresectable disease, nano-knife (irreversible electroporation) surgery is the preferred option, with outcomes far superior to those of other conventional therapies. Biliary stenting via endoscopic or percutaneous transhepatic approaches can be performed to relieve jaundice. Image-guided radiofrequency ablation or microwave ablation may be used for local disease control. Radioactive seed implantation can be employed to deliver brachytherapy to localized lesions.
· Chemoradiotherapy: Concurrent chemoradiotherapy is used for local control in locally advanced disease, while chemotherapy serves as the foundation of first-line treatment for advanced-stage disease.
· Targeted and immunotherapy:PARP inhibitors are used for BRCA-mutated tumors; immune checkpoint inhibitors are indicated for select patient populations.
· Other treatments:Biliary drainage, nerve block analgesia, and nutritional support improve quality of life.
Contrast-enhanced CT is the imaging modality of first choice, with MRI/MRCP serving as an adjunct for evaluating the biliary and pancreatic ducts. Endoscopic ultrasound-guided biopsy confirms the diagnosis. CA19-9 is an important tumor marker, and PET-CT is used to assess metastatic disease.