Melanoma is highly aggressive. In China, acral lentiginous melanoma accounts for a relatively high proportion, differing from the predominant cutaneous type in the West. In recent years, advances in immunotherapy and targeted therapy have significantly prolonged survival in advanced patients.
· Intense sun exposure and history of sunburn
· Fair skin, multiple moles, and atypical nevi
· Family history of melanoma
· Immunosuppressed state
· Tanning bed use and ultraviolet exposure
Ultraviolet radiation induces characteristic mutations such as BRAF V600E, activating the MAPK pathway and causing malignant proliferation of melanocytes. Acral melanoma is often not UV-dependent and is driven by gene rearrangements/amplifications. Immune escape is key to progression.
Cutaneous melanoma presents as ABCDE changes in moles (asymmetry, border irregularity, color variegation, diameter >6 mm, and evolution/enlargement). Acral melanoma occurs on the palms, soles, or as longitudinal pigmentation under the nails. Regional lymph nodes may enlarge, and distant metastases cause corresponding symptoms.
· Surgery: Wide local excision plus sentinel lymph node biopsy forms the basis of curative treatment, with surgical margins determined by depth of invasion.
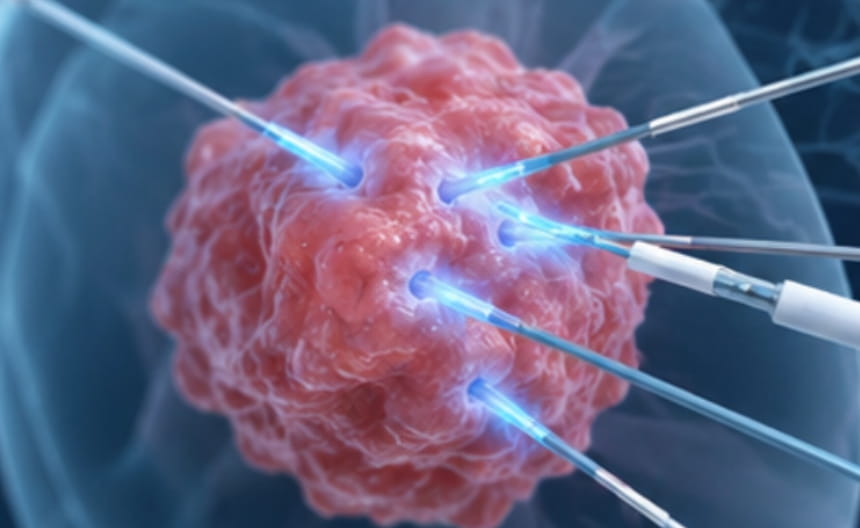
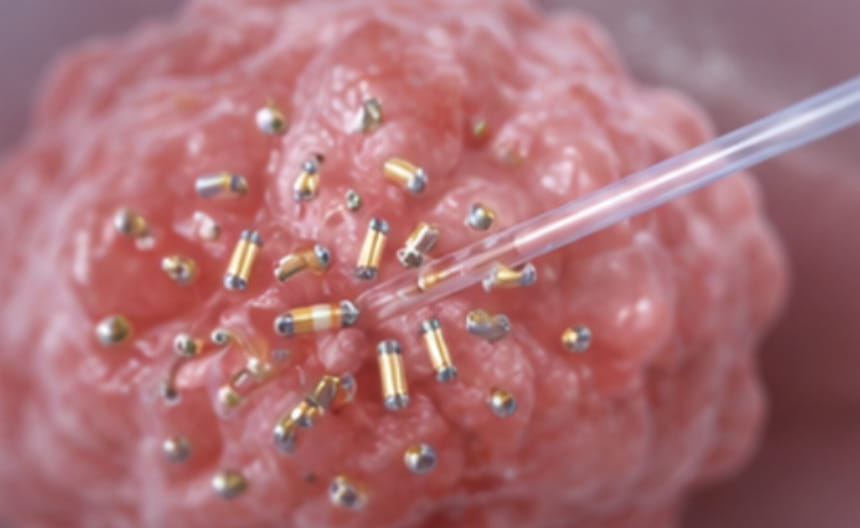
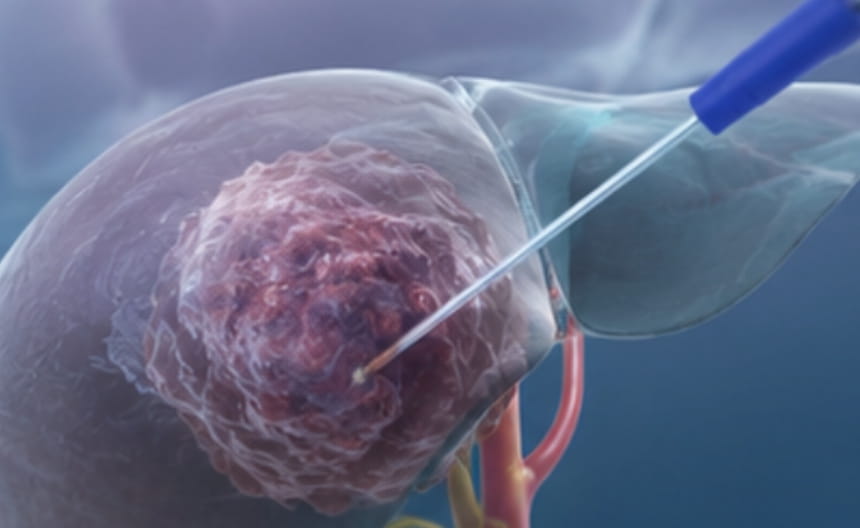
· Minimally invasive treatment: Isolated subcutaneous or visceral oligometastatic lesions may be precisely destroyed by image-guided radiofrequency ablation, microwave ablation, or cryoablation; intratumoral immunotherapy-like injections may also be used for skin metastases.
· Chemoradiotherapy: Radiotherapy is used for palliative pain relief and local control of bone and brain metastases; chemotherapy is used in later lines.
· Targeted and immunotherapy: Combined BRAF/MEK targeted therapy is used for patients with BRAF mutations; immune checkpoint inhibitors, alone or in combination, are the preferred first-line treatment for advanced disease and can achieve long-term survival.
· Others: Lifelong skin self-examination and follow-up, and ultraviolet protection measures.
Dermoscopy improves diagnostic accuracy, and full-thickness excisional biopsy is the gold standard. BRAF mutation testing is required. Ultrasound and whole-body PET-CT are used for staging. Close postoperative follow-up of the skin and regional lymph nodes is required.