Cervical cancer is a malignant tumor that seriously threatens women's health and is almost 100% associated with persistent infection by high-risk human papillomavirus (HPV), with squamous cell carcinoma being the most common histological type. The progression from HPV infection to cervical intraepithelial neoplasia and eventually to invasive carcinoma usually takes 10–20 years, providing a valuable window for screening and intervention. The successful development of HPV vaccines has made cervical cancer the first—and currently the only—cancer that can potentially be eliminated. Even after diagnosis, the cure rate for early-stage cervical cancer can exceed 90%, while standardized radiotherapy and systemic therapies can significantly improve survival outcomes in patients with advanced disease.
· Persistent infection with high-risk HPV types (HPV 16 and 18 account for approximately 70% of cervical cancers)
· Multiple sexual partners or early age at first sexual intercourse
· Multiple childbirths and smoking
· Immunosuppression (e.g., HIV infection or post-organ transplantation status)
· Long-term use of oral contraceptives (risk increases after more than 5 years of use)
· Low socioeconomic status and lack of regular screening programs
High-risk HPV integrates its E6 and E7 oncogenes into the genome of host cervical epithelial cells. The E6 protein promotes ubiquitin-mediated degradation of the tumor suppressor p53, while the E7 protein inactivates the retinoblastoma (Rb) protein, leading to uncontrolled cell-cycle progression and marked genomic instability. Concurrently, the virus evades immune surveillance, enabling persistent infection and the stepwise accumulation of genetic mutations that ultimately drive malignant transformation. Synergistic factors such as smoking further exacerbate DNA damage and suppress local immune responses, thereby accelerating carcinogenesis.
Early-stage cervical cancer often causes no noticeable symptoms. The most characteristic symptom is postcoital (contact) bleeding, which refers to light vaginal bleeding after sexual intercourse, a gynecological examination, or straining during defecation. Other manifestations may include intermenstrual bleeding, increased menstrual flow, prolonged menstrual periods, postmenopausal bleeding, and increased vaginal discharge, which may be watery, blood-stained, or purulent with a foul odor. As the disease progresses, tumor invasion of the pelvic wall can lead to persistent pelvic and lumbosacral pain. Compression of the ureters may result in hydronephrosis, while vascular compression can cause lower-extremity edema. In advanced cases, vesicovaginal fistulas or rectovaginal fistulas may develop.
· Surgery: For patients with early-stage cervical cancer (FIGO stages IA–IB1), treatment options include simple (extrafascial) hysterectomy or radical hysterectomy with pelvic lymph node dissection. For young patients with early-stage disease who wish to preserve their fertility, radical trachelectomy with preservation of the uterine body may be performed. Minimally invasive laparoscopic techniques can also be used to reduce surgical trauma and facilitate recovery.
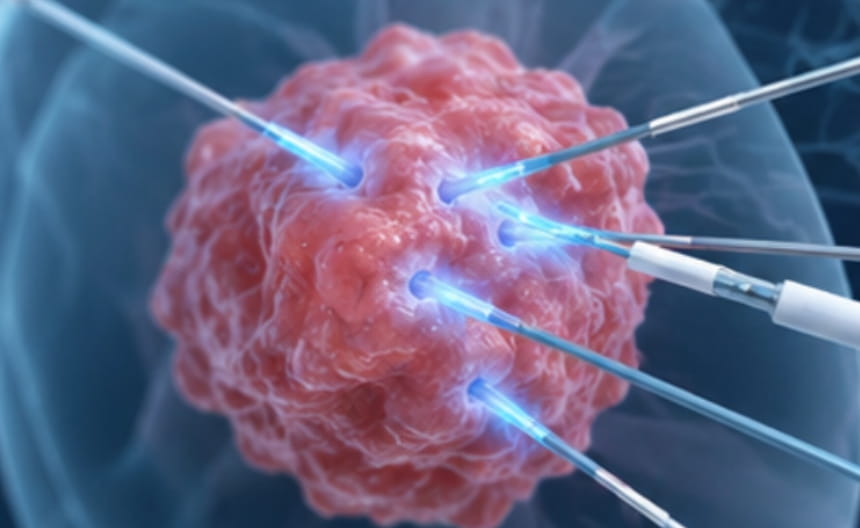
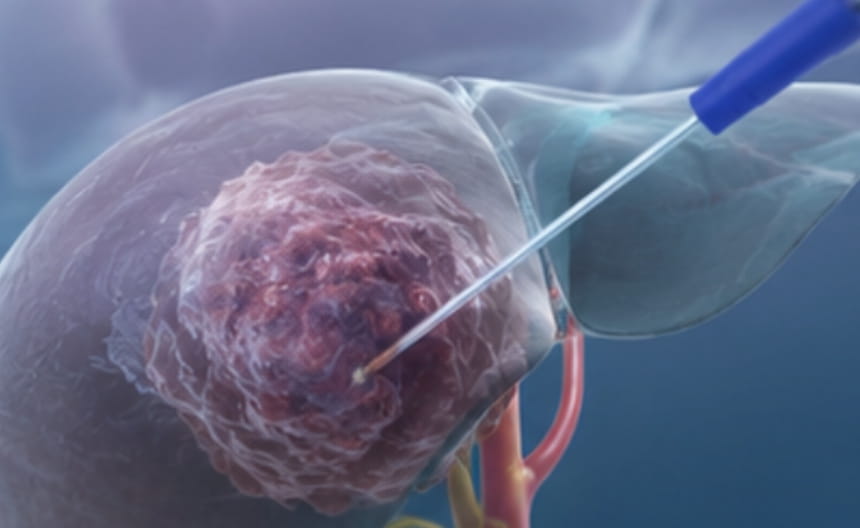
· Minimally invasive therapy:Conization and Local Ablation Therapies: The loop electrosurgical excision procedure (LEEP) and cold-knife conization (CKC) can completely remove cervical precancerous lesions and microinvasive cervical cancer while preserving fertility. For selected patients with isolated recurrent or metastatic lesions, image-guided radiofrequency ablation (RFA) or cryoablation may be used to achieve effective local tumor control.
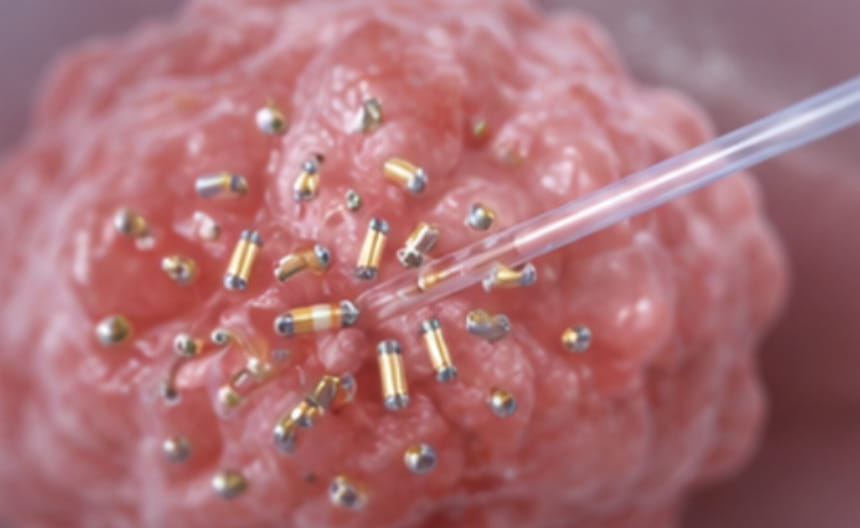
· Chemoradiotherapy: Radiotherapy and Concurrent Chemoradiotherapy: For locally advanced cervical cancer, the standard treatment is pelvic external beam radiotherapy (EBRT) combined with platinum-based concurrent chemotherapy and supplemented by intracavitary brachytherapy, with curative intent. Radiotherapy is also widely used as adjuvant treatment for patients with high-risk pathological features after surgery. In advanced-stage disease, it can provide palliative symptom relief, particularly for pain control and the management of metastatic lesions.
· Targeted and immunotherapy: Targeted Therapy and Immunotherapy: The combination of anti-angiogenic targeted therapy and chemotherapy is a standard first-line treatment option for recurrent or metastatic cervical cancer. In addition, immune checkpoint inhibitors have demonstrated durable clinical responses in patients with PD-L1–positive or microsatellite instability-high (MSI-H) advanced cervical cancer, offering a promising therapeutic option for selected patients.
· Other treatments: Prevention and Supportive Care: HPV vaccination for eligible individuals is the most effective and fundamental strategy for preventing cervical cancer. In addition, psychological support, pelvic floor rehabilitation therapy, and ovarian preservation or protection measures can help improve quality of life, reduce treatment-related complications, and support long-term physical and emotional well-being.
Liquid-based cytology combined with high-risk HPV DNA testing is an internationally recognized standard screening strategy. For individuals with abnormal screening results, colposcopy is performed, and multiple biopsies are taken from suspicious areas, or diagnostic cervical conization is carried out. Clinical staging is based on gynecological examination, supplemented by MRI, CT, or PET-CT. Molecular subtyping, including gene expression profiling, provides a reference for prognostic assessment and precision treatment.